Purpose and Applicability
Isoflurane gas is commonly used as an inhalation anesthetic in animal research. It is a clear, colorless, volatile liquid at room temperature and pressure. Exposure to second-hand anesthetic gases has been associated with several health concerns and can occur when vapors escape into the work environment during the administration of anesthesia. Since these gases are odorless and have very poor warning properties, there is no indication when an exposure to these substances is occurring. This guideline will focus on the use of isoflurane when administered to research animals. This generic chemical safety guidance describes basic prudent safety practice for handling this chemical in research labs. The principal investigator (PI) or the lab manager is responsible for developing and implementing standard operating procedures (SOPs) for the purchase, storage, and safe handling of this chemical that are specific to the PI’s research.
Contact information and areas of expertise can be found on the Contact Us page
Hazards
Isoflurane is an eye and skin irritant and central nervous system toxicant. Long-term exposure may cause chronic or adverse health effects including nausea, dizziness, fatigue, headache, irritability, reduced mental performance, liver and kidney disease, and possible reproductive effects (sterility, infertility, miscarriages, and birth defects). Inhalation of isoflurane at high concentration levels (at or above 3%, v/v in air) may lead to death.
Handling.
Exposure Risks:
Based on evaluations done at numerous institutions, the following activities have been found to have an increased risk of exposure:
- Not ensuring a tight seal around the animal’s nose cone;
- When using a nose cone to deliver the anesthetic gas, make sure to achieve a tight seal around the animal’s nose for rodents and rabbits or, for all other animals, around the animal’s nose and mouth.
- Failing to flush the induction chamber with oxygen prior to opening the chamber to transfer animals;
- When purging the induction chamber via the oxygen flush button, use an appropriate scavenging system to ensure no WAG escapes into the workspace.
- Performing multiple animal surgeries, requiring an extended length of time that anesthesia is delivered.
Upon request, EHS will evaluate staff exposures by monitoring laboratory workers while they perform work with isoflurane.
Exposure Limits
The American Conference of Governmental Industrial Hygienist (ACGIH) has established a non-regulatory occupational exposure limit for isoflurane of 50 ppm as an 8-hour time weighted average. OSHA has not established a regulatory permissible exposure limit (PEL) for isoflurane; therefore, 50 ppm is used as the exposure limit.
Since each lab’s research and environmental conditions vary, it is recommended that exposure monitoring is performed at least one time to ensure isoflurane levels are less than 50 ppm.
Safety Equipment
Approved Scavenging Methods
Potential exposure routes include inhalation and skin contact. It is extremely important to control and minimize any leaks of isoflurane vapor. Waste anesthetic gas (WAG) must be scavenged through active or passive means. Active scavenging involves an active airflow system that draws WAG away from the researcher into an in-house WAG exhaust line, chemical fume hood, canopy hood or snorkel. Passive scavenging methods involves passing the WAG through an activated charcoal canister, after which it is discharged into the room. To reduce the risk of exposure to escaped vapors, one of the following control measures should be in place when administering anesthesia:
- First Choice: Use of a downdraft surgery table or if space/procedure allows, placement of the entire gas mixing and delivery system within a fume hood (this is not appropriate for aseptic surgery procedures) or use of an in house WAG exhaust line.
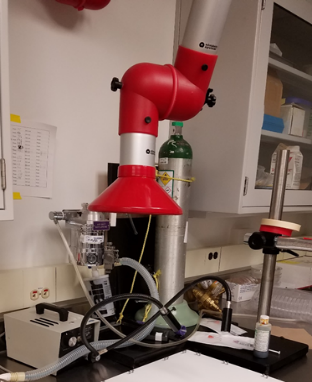
- Second Choice: Installation of local exhaust over the isoflurane delivery system to address a single source of anesthetic gas, similar to that shown in the photo to the right, or a slot or canopy exhaust for procedures that involve multiple sources of anesthetic gas (e.g., induction box, procedure table, etc.).
- Third Choice: Capture of waste gas using gas scavenging canisters. The work must be done in a well-ventilated area with no recirculation of room exhaust. Scavenging canisters are appropriate under the following conditions:
- No fume hood or other local, hazardous exhaust system is available for use;
- Leak checks are performed routinely on equipment;
- Saturation levels of canisters are checked prior to each use; and
- Researchers are trained and supervised in proper use and maintenance of the anesthetic equipment. If not properly used or maintained, gases may escape into the work area resulting in overexposures.
Notes on use of gas scavenging systems:
Absorption canisters with exhaust ports located on the top alleviates back pressure, resulting in better capture. Absorption canisters with exhaust ports on the bottom should be raised such that the vents are not blocked (see basket use with F/AIR canister, below). Either type of canister should be used in the manufacturer’s recommended position.


Decreasing oxygen flow to the lowest effective rate during anesthetic gas administration can also reduce the concentration of waste gases in the work environment. For example, reducing the oxygen flow rate for a single mouse can still anesthetize the mouse while reducing the concentration of waste gases in the work environment to more acceptable levels.
Equipment Calibration and Maintenance: Contact the equipment supplier or authorized technician regarding proper handling of isoflurane equipment, annual calibration and maintenance, and leak/pressure testing of an anesthetic machine. Per IACUC Guidelines: Anesthesia annual calibration for vaporizers is required unless the manufacturer states that calibration is not required (e.g. – Kent Scientific Somno Suite).
Personal Protective Equipment
Nitrile gloves, lab coats and eye protection (safety glasses, goggles or a face-shield) should be worn to prevent contact with liquid anesthetic gases.
Note: N95 or R95 dust masks are not to be used as either primary or secondary respiratory protection from isoflurane exposure. If a researcher would like to use a tight-fitting elastomeric respirator, please contact Justin Newnum at 335-9554 to evaluate the hazards through exposure assessment sampling to determine what, if any, respirator must be used, or if a voluntary respirator program is appropriate.
Dust masks however may be used for protection against animal allergens.
Prudent Practices
- Stock bottles of isoflurane should always be kept in a cabinet in a ventilated room.
- Use a cylinder cart to move gas cylinders from one location to another. Use of ‘spin-and-roll’ or dragging cylinders is unacceptable.
- Check the integrity of the pressure gauge connected to the compressed gas cylinder.
- Check the flow meter control valves regularly and ensure the flow indicator does not stick to the burette and deform the burette wall.
- Check the integrity of gaskets to prevent the occurrence of isoflurane leaks, especially when using an induction chamber.
- If using, place the WAG canister in the manufacturer’s recommended position, ensuring exhaust ports are not blocked/covered. Ensure the canister has not exceeded the required absorption weight prior to starting a procedure. Depending on the length of procedure, the oxygen flow rate and the isoflurane concentration, you may need to weigh the canister during the procedures as well.
- Induction chambers:
- A laboratory-specific standard operating procedure (SOP) should include purging the induction chamber with oxygen before opening it and then removing the animal. Ensure the vent port from the induction chamber is connected to a WAG charcoal canister, when a scavenging system is used.
- If the induction chamber has a hinged lid, position it and the isoflurane away from your breathing zone.
- EHS recommends using an induction chamber with a slide-top lid (e.g., vapor-vac hooded induction chamber, see Patterson Scientific) as opposed to an induction chamber with a hinged lid to minimize WAG exposure.
- Isoflurane drop jars must be kept within a fume hood and the sash closed to as minimal of an operating height as possible (at least below the user’s chin) to prevent isoflurane exposure.
- Leak testing for isoflurane should be routinely performed by laboratory staff.
- All plastic tubing (e.g., silicone, PVC, and Tygon) should be checked periodically for weathering, discoloration, etc., and replaced as needed.
- Purchase and maintain an isoflurane spill kit.
- Following a major spill, staff should immediately exit the room and prevent others from entering the room until the spill has evaporated. Exposure to isoflurane can occur when staff try to wipe up spilled isoflurane with towels, thus coming into close proximity with the chemical.
Spill/Exposure Procedures
Eyes: If anesthetic gases/liquids come into contact with eyes, immediately flush them with copious amounts of water for at least 15 minutes, preferably in an emergency eyewash.
Skin: In the event of skin exposure, remove contaminated clothing and immediately wash the affected area with soap and water.
SIGNS & SYMPTOMS of Isoflurane Exposure
- Acute Exposure: nausea, vomiting, skin and respiratory irritation, including the nose and throat, headache, dizziness, and drowsiness
- Chronic Exposure: hypotension, tachycardia, respiratory depression, elevated blood glucose
If any of these symptoms appear, seek immediate help from the UI Occupational Health or the UIHC Emergency Treatment Center.
Waste Disposal
Disposal of absorbent canisters that contain activated carbon to prevent release of the anesthetic gas to the environment must be managed as hazardous chemical waste. EHS provides waste collection services; complete a Chemical Waste Pickup Request form to have canisters collected for proper disposal. To manage the used canisters while awaiting pickup, label the canisters as hazardous waste and store them in a sealed plastic bag or plastic box to avoid off gassing into the room.
Training
The PI is responsible for SOPs specific to use of this chemical in their lab. The PI/Lab Manger is responsible for the site specific and hands-on training for the use of this chemical in their lab. Training should be directly documented in the researcher’s lab notebook. On each day of training, both trainer and trainee should sign the lab notebook.
Initially, researchers should perform the reactions with the PI or senior researcher present to observe the safe handling of this chemical. Review the reagent-specific safety data sheets (SDSs). Evaluate the hazards associated with the chemical reaction and experimental setup.
Resources
External Links
OSHA Guidance Document – ANESTHETIC GASES: Guidelines for Workplace Exposures